.png "Call Us")





it’s a blank canvas
so full of opportunities
WOWEE
ADA RESEARCH BRIEF
Health Care Access and the ADA
The Americans with Disabilities Act (ADA) passed on July 26, 1990. It provides a legal framework for people with disabilities to challenge discriminatory practices in work settings, state and local government, and places of public use. Under the ADA, disability is formally recognized as a source
What is
of discrimination, similar to how “race, color, religion, sex, or national origin” is recognized by the Civil Rights Act of 1964. The ADA’s importance extends well beyond the court system. The ADA is also a broader symbol of bipartisan support for disability inclusion in all parts of public life. The larger goal of the law is to assure equality of opportunity, full participation, independent living, and economic self-sufficiency for all individuals with disabilities.
the ADA?
Research
Highlights
Barriers to health care are not limited to times when people with disabilities are receiving health care.
While the ADA does not include specific language, Titles II & III of the ADA continue to provide protection from discrimination in emergencies.
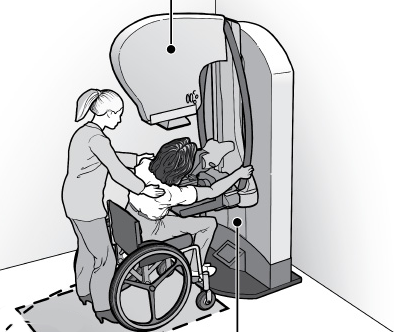
Lack of accessible medical equipment and devices prevents people with disabilities from getting adequate health care and services and can jeopardize patient safety.
Health care professionals need more opportunities to learn beyond physical accessibility and compliance with the ADA.
Inaccessibility also affects medical professionals with disabilities that encounter barriers to access.
GETTING IN THE DOOR
ADA-related barriers to accessing health care begin before people with disabilities even reach the door.
HEALTH CARE ACCESS BARRIERS
Transportation
Parking
Accessibility of the building
Emergency & preventative services
Primary care
Barriers have been shown to be similar cross-disability, regardless of disability type.
EMERGENCY & DISASTER
PREPAREDNESS
While the ADA does not include specific language, Titles II & III of the ADA continue to provide protection from discrimination in emergencies.
Men with disabilities are 19% less likely to report getting prostate-specific screening test.
64.6% of women with disabilities reported receiving pap tests compared to 82.5% of women without limitations.
61.4% of women with disabilities reported having mammograms compared to 74.4% of women without impairments.
CONSEQUENCES OF BARRIERS TO ACCESSING HEALTH CARE
SOCIAL
PSYCHOLOGICAL
Social consequences have to do with relationships, individual social roles, and social participation.
Psychological consequences often involve depression, frustration, and stress along with experiences of devaluation.
PHYSICAL
ECONOMIC
Physical consequences may lead to a deterioration in one’s health due to lack of access to preventive, diagnostic, or other health care.
Economic consequences involve potential lost wages, financial strain, and additional health service costs that one must undertake.
MEDICAL EQUIPMENT
and Devices
Lack of accessible medical equipment and devices prevents people with disabilities from getting health care and services
and can risk patient safety.
CLICK HERE
EXAMPLES OF EQUIPMENT :
To learn more about accessible
medical equipment and devices.
BUT...
It's not just about physical access
People with cognitive disabilities experience barriers that can be addressed by adjusting procedures to accommodate for their needs.
Health care providers are required to provide full and equal access to services and facilities under Titles II and III of the ADA.
REASONABLE
MODIFICATIONS
Changes policies, practices, and procedures must be made as necessary to ensure health care services and facilities are fully accessible, unless such modifications would “fundamentally alter” the nature of the services.
HEALTH CARE PROVIDER
Knowledge
46% of health care administrators in clinical practices knew accessible equipment existed.
25.4% were able to describe accessible equipment.
44% of administrators had considered purchasing accessible equipment at some point.
Only 22% knew of the federal tax credit program that assists businesses in complying with the ADA.
Pharr, J. (2013). Accessible medical equipment for patients with disabilities in primary care clinics: Why is it lacking? Disability and Health Journal, 6(2), 124-132
Research found there is a significant correlation between knowledge about accessibility and accessible equipment being provided in health care clinics:
PROVIDER PREDICTORS OF HEALTH CARE ACCESS BARRIERS
Age of practice administrator
Number of years working (i.e. experience with the ADA)
Buildings built before 1993 must be modified to comply with the ADA
Lack of administrator knowledge of the ADA
Health care professionals need more opportunities to learn beyond physical accessibility and compliance with the ADA. Disability needs to be an integral part of education and training for health care professionals.
One promising strategy is to involve people with disabilities in training and developing materials for future health care professionals.
MEDICAL PROFESSIONALS
with Disabilities
Title III of the ADA provides for public accommodations, including universities and medical schools. However, most medical schools fall short on providing reasonable accommodations to students with disabilities under the ADA.
77% of medical schools technical standards do not explicitly mention accommodating students with disabilities.
There is a systematic exclusion of students with disabilities in medical and nursing schools.
Over 90% were biased against intermediaries that would allow some students with disabilities to succeed.
Inaccessibility also affects medical professionals with disabilities who encounter barriers. Title I of the ADA prohibits discrimination on the basis of disability in employment, including individuals who work in health care settings.
KEY ISSUES FACING MEDICAL PROFESSIONALS WITH DISABILITIES
Job accommodations
Perceived attitudes of colleagues and supervisors
Physical access barriers in the facilities within which they do work
STRATEGIES FOR INCLUSION
Recommended by the University of Pennsylvania
Strategize to address non-physical barriers.
Strategize to address physical barriers.
Develop different pathways in evaluation and promotion.
Strategize to provide reasonable accommodations.
FOR MORE INFORMATION CONTACT:

This information product was developed under a grant from the Administration for Community Living (ACL) NIDILRR grant number 90DP0086. However, the contents do not necessarily represent the policy of ACL and you should not assume endorsement by the Federal Government.
SUGGESTED CITATION: Gould, R., Parker Harris, S., Caldwell, K., & Mullin, C. (2018). ADA Research Brief: Health Care Access and the ADA (pp. 1-3). Chicago, IL: ADA National Network Knowledge Translation Center.